Cause
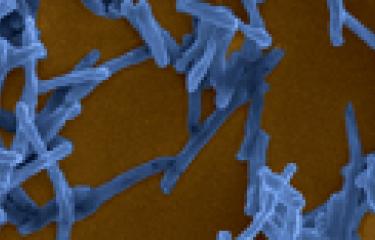
The infectious agent responsible for Buruli ulcer is Mycobacterium ulcerans. Unlike other species of the Mycobacterium genus, this bacterium produces a toxin known as mycolactone. Its pathogenicity can be attributed to this toxin. Although the mode of disease transmission remains poorly understood, it is thought that the infection may be transmitted through contact between skin lesions and contaminated water or through bites from insect vectors.
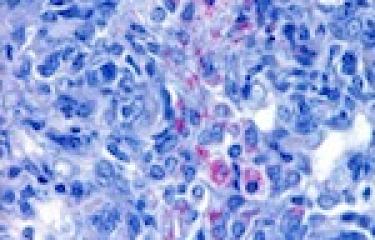
Symptoms
Buruli ulcer is not a fatal disease. The bacteria multiply in skin and mycolactone production results in ulceration of surrounding tissue, potentially leading to major, irreversible skin lesions. These ulcers are painless as the toxin has analgesic and anti-inflammatory properties.
Epidemiology
According to estimates, the disease affects several thousand people per year. However, it is likely that the actual figures are higher. Although the main focus of the disease is West Africa, it is also observed in America, Asia and the Western Pacific. The World Health Organization (WHO) classifies it as a neglected tropical disease and reviews the situation regarding this infection every two years.
Treatment
Buruli ulcer is treated by 8 weeks of combination antibiotic therapy taken on a daily basis with skin grafts in case of extensive lesions. The antibiotic therapy is difficult to monitor and surgery is difficult to perform given conditions in the field. Research on improving control of Buruli ulcer is focused on understanding the mode of transmission, developing early diagnostic tests, identifying more effective and therefore shorter treatments, and developing vaccines.
June 2021